|
by Eun Myoung Shin and Alan Prem Kumar
  reast cancer is a cancer that starts in the tissue of the breast. There are two main types of breast cancer based on which part of breast tissue becomes cancerous (Figure 1). Ductal carcinoma starts in the tubes that move milk from the breast to the nipple. Most breast cancers are of this type. Lobular carcinoma starts in the parts of the breast that produces milk. In rare cases, breast cancer can starts in other areas of the breast. Men can get breast cancer though women are 100 times more likely to get breast cancer than men. Breast cancer is a complex and heterogeneous disease whose evolution is difficult to predict. Incidence rates of breast cancer have been increasing throughout the world. Breast cancer ranked the fifth, after lung, stomach, liver, and colon cancers, causing 460,000 deaths in 2008 according to World Health Organization Medica Center "Cancer" 2011 [1]. reast cancer is a cancer that starts in the tissue of the breast. There are two main types of breast cancer based on which part of breast tissue becomes cancerous (Figure 1). Ductal carcinoma starts in the tubes that move milk from the breast to the nipple. Most breast cancers are of this type. Lobular carcinoma starts in the parts of the breast that produces milk. In rare cases, breast cancer can starts in other areas of the breast. Men can get breast cancer though women are 100 times more likely to get breast cancer than men. Breast cancer is a complex and heterogeneous disease whose evolution is difficult to predict. Incidence rates of breast cancer have been increasing throughout the world. Breast cancer ranked the fifth, after lung, stomach, liver, and colon cancers, causing 460,000 deaths in 2008 according to World Health Organization Medica Center "Cancer" 2011 [1].
Cancer risk varies geographically and across ethnic groups that can be monitored in cancer control to respond to observed trends as well as ensure appropriate health care. According to a study reviewing 37 previous studies published between 1990 and April 2010 focusing on cancer in adult migrants from non-western countries, living in the industrialized countries of the European Union revealed that migrants from non-western countries were more prone to cancers that are related to infections experienced in early life, such as liver, cervical and stomach cancer. In contrast, migrants of non-western origin were less likely to suffer from cancers related to a western lifestyle, such as colorectal, breast and prostate cancer [2].
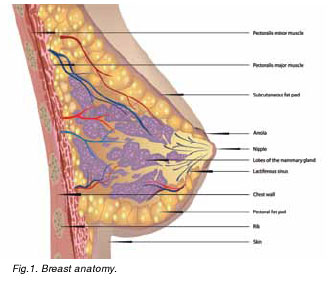
As Asian countries become increasingly westernized, incidence rate will increase for many cancers. Presently, breast cancer incidence rate is considerably lower than in Western countries, however, breast cancer risk has been ever increasing in most Asian countries. The age-standardized incidence rates of breast cancer had been increasing from 32.5 per 100,000 in 1983 to 35.0 per 100,000 in 2004 and further increased to 45.9 per 100,000 in Fig.1. Breast anatomy.2008[1]. Rapid urbanization, improvement in socio-economic status of women, and adaption of a western lifestyle can be possible explanations. In female, incidence of breast cancer ranked first in Taiwan, China, Singapore, Japan and India with the highest incidence (53.7 per 100,000) of breast cancers is in Manila, Philippines [1].
There are differences in incidence rates and trends between Caucasians and Asian populations suggesting further detailed research in enlightening the epidemiology of breast cancer in Asians be presented [3]. In Asian female, the incidence rates plateau in the middle age and declined in the older age with the mortality rates consistently increasing with age. The patterns of age-specific mortality during the last three decades in Hong Kong and Singapore gradually increases with age, while Japan, Korea and Taiwan showed rather flat or declining after age 50. Mortality rates by age group showed that for the woman aged 35-49 and 50-69 years, the rate has been increasing significantly in recent years in Japan, Korea, and Taiwan but decreasing in Hong Kong and Singapore [1, 4].
Despite the increasing incidence of and mortality from breast cancer, Asian women in the United States of America report consistently low rates of mammography screening. A number of health beliefs and sociodemographic characteristics have been associated with mammogram participation among these women. A cancer incidence and survival in Asian Indian-American patient study showed that the median age at diagnosis was 52 (range 25-79) and the median tumor size was 1.5 cm (range 0.2-4.5 cm). Differing from their Caucasian counterparts, Asian Indian-American women were more likely to present with palpable masses and at a younger age. This may indicate a social or cultural barrier to routine screening mammograms and possibly a biologically more aggressive tumor [5].
Breast cancer can be defined at the clinical, histological, cellular and molecular levels. In order to understand and refine the breast cancer taxonomy, from the initial histological features such as tumor size, tumor grade, lymph node status and the presence of predicative markers such as estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor-2 (HER2) status to a further sophisticated classification of luminal A, luminal B, HER-2 positive, basal-like and the normal subtypes have been established to facilitate cancer treatments. Over the decade, this profiling has contributed significantly to our understanding of this heterogeneity at the molecular level. Gene expression profiling studies have further identified several breast cancer subtypes associated with markedly different clinical outcomes. Currently, hormonal therapy is prescribed to patients with ER positive breast cancer. In principle, the estrogen antagonist Tamoxifen is used to block the effects of estrogen, which can help ER positive breast cancer cells survive and grow. Another class of hormonal therapy medicines called aromatase inhibitor, such as exemestane (Aromasin) blocks estrogen from being made. For the HER2 positive breast cancer patients, HER2 targeted treatment trastuzumab (Herceptin) can be used. On the other hand, chemotheraphy is currently the mainstay of systemic treatment for ER negative, progesterone negative and HER2 negative subtypes (triple negative subtype) of breast cancer due to hormonal and HER2-directed therapies are not effective. The overall poor prognosis of patients with triple negative breast cancer and/or basal-like breast cancer and their tendency to relapse with distant metastases indicate a definite need for effective systemic therapies for this disease. Chemotherapy for the treatment triple negative breast cancer and basal like breast cancer have been trying diversified strategies so far. Several PARP inhibitors are in phase II/III development and angiogenesis inhibitor bevacizumab, which targets VEGF, is currently under investigation both in triple negative breast cancer patients and in patients with metastatic breast cancer in combination with a taxane. The anti-diabetic drug metformin has been shown to inhibit proliferation and induce apoptosis of triple negative breast cancer in preclinical studies, in addition to inducing other beneficial biological changes in breast cancer of various types. Clinical trials for EGFR inhibitors are also being evaluated in triple negative breast cancer patients. Tyrosine kinase c-src is another therapeutic target in breast cancer since c-src is associated with increased motility and invasiveness in breast cancer [6]. Encouraging results have been reported, yet preclinical and clinical trials are still on the process and there are little prospective data at current time.
Triple negative breast cancers occurred 2-3 times more frequently in African American patients (up to 47% of breast cancers), the percentage of triple negative breast cancers was 55% in West-African patients, 31% in Korean patients, 18% in Chinese patients and 16% in Taiwanese patients, and 8% in Japanese patients[6]. In Asian countries, Korea showed the most rapid increases in breast cancer mortality for all age group with the highest triple negative rate in Asia. A medical record review study of 683 patients consisted of 136 triple negative breast cancer and 529 non-triple negative breast cancer cases showed that triple negative breast cancer correlated with younger age (< 35 years), and higher histologic and nuclear grade in Korean cohort. It also correlated with a molecular profile associated with biological aggressiveness: negative for bcl-2 expression, positive for the epidermal growth factor receptor, and a high level of p53 and Ki67 expression. Relapse free survival was significantly shorter among patients with triple negative breast cancer compared with those with non-triple negative breast cancer [7]. Apart from that patients with triple negative breast cancer were more likely to develop distant metastasis earlier, and also evidenced poor overall survival. Triple receptor status may be employed as a prognostic marker for breast cancer patients with brain metastases [8]. Similarly, basal-like triple negative breast cancers are associated with adverse clinicopathologic parameters, and that individual biologic markers of CK17, CD117, and SMA have prognostic implications on survival. Possibilities exist for future targeted therapy for this challenging group of breast cancers [9].
In summary, however, according to a review study of 1018 breast cancer patients in Canada, the differences in survival and prognostic factors between patients with triple-negative breast cancer and those with non-triple negative breast cancer was insignificant. The significant predictors of survival in the adjusted analysis were age, stage of cancer, and size of cancer, indicating that presenting tumor size at diagnose is the most important prognostic factor in triple negative breast cancer. Investigations into unique screening methods to identify these tumors at an earlier stage and to prevent advanced-stage cancer in this patient subpopulation are necessary. Late stage at diagnosis was largely responsible for low survival.
In Western countries, mortality started to decline due in part to birth cohort effects for women born from the end of 19th century to the mid-1920s and the decline is further expected to continue in this decade due to the long term result of both mammography screening and improved medical intervention [4]. Medical services for breast cancer patient management have reached the quality standards in the guidelines in Asian countries since 1990s. Taiwan started a stratified breast screening program in 1995. Singapore, Japan and Korea organized breast cancer screening program in 2002 that combines mammography with clinical breast examination. European countries which started breast screening program in early 1990s have experienced decline in the breast cancer mortality rate [4]. Early detection and treatment improvement will continue to reduce the mortality rates as observed in Western countries. However predominant early onset and aggressive ER-negative breast cancers may still partially account for the high breast cancer mortality in Asian countries.
 Click here to download the full issue for USD 6.50 Click here to download the full issue for USD 6.50
|