|
by David E. Goldberg
 sia consists of almost 50 countries with approximately 4 billion people, making up 60 per cent of the worlds population. With a population that has been rising faster than Europes or Americas, the proportion of people over 65 years of age is also on the rise. sia consists of almost 50 countries with approximately 4 billion people, making up 60 per cent of the worlds population. With a population that has been rising faster than Europes or Americas, the proportion of people over 65 years of age is also on the rise.
As the countries in Asia become more developed, its population has adopted a more Westernised lifestyle, dietary change with increasing fat, red meat and alcohol consumption, alongside with established habits like smoking. This, combined with the increasing and aging population and fewer deaths from infectious diseases, has increased the rates of cancer in Asia. Asias prevalence of cancer deaths may climb 45 per cent to 163 per 100 000 people by 2030, from about 112 per 100,000 in 2005, according to the World Health Organization. At that rate it would overtake the rates in the United States, where cancer-related mortalities are expected to rise to 156 per 100,000 from 136 per 100,000 over the same period. Therefore, cancer is emerging as one of the most important health problems in Asia. Accordingly, cancer prevention and screening have emerged as important issues in each Asian countrys health program (1-3).
Asia covers a vast geographical area, and can be divided into regions Central, East, West, South and South East Asia. As the regions vary greatly in their ethnic groups, cultures and traditions, social and economic status, there is great geographical variation in cancer demographics.
Main Cancers in Asia
In East Asia, the leading cancers with the highest incidence rates are lung cancer, followed by stomach, liver and colorectal cancers. In Central and South Asia, the main cancers are cervical uteri, breast, lung and lip/oral cancers. In West Asia, breast, lung, colorectal and stomach cancers are the leading cancers. In South East Asia, lung, followed by breast, liver and colorectal cancers have the highest rates.
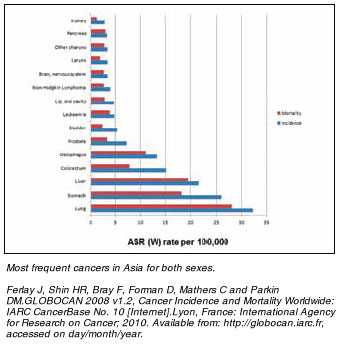
In terms of mortality, lung cancer is the most common cause of cancer death in Asia, followed by colorectal, breast, liver and stomach cancers (Figure1).
Lung Cancer
Tobacco use is the single greatest risk factor in lung cancer. The habit of cigarette smoking is prevalent in Asia. Tobacco advertisements are common sights in Asia. China is the worlds largest tobacco production and consumption country. An estimated 300 million men in China are smokers, with many more people being exposed to second hand smoke. The average age to start smoking in China is decreasing from age 22 in 1984 to 19 in 1996 and to 18 in 2002 (4). The trend of an earlier starting age of smoking is worrying. The WHO estimated that by 2025, more than 1,000,000 Chinese will be diagnosed with lung cancer alone each year. Smokeless tobacco is also a big problem in India, where many men and women chew some form of tobacco. Adenocarcinoma characterized by mutations in the activating domain of the epidermal growth factor receptor, is distinguished by its association with light or never smokers, and female preponderance, and more common in East Asia than the rest of the world.
Colorectal Cancer
There is geographical variation in the incidence of colorectal cancer in Asia. This can be attributed to differences in diet, particularly with the consumption of red and processed meat, fibre and alcohol, as well as bodyweight and physical activity. Incidence rates of colorectal cancer are increasing in countries where rates were previously low, such as Japan, as diets become Westernised (5).
Breast Cancer
Breast cancer is the most common cancer diagnosed in women in Asia, with incidence generally higher in the developed countries and lower in developing countries. Reproductive behaviour and the use of exogenous hormones, as well as differences in weight, exercise, diet and alcohol consumption are probable reasons for the differences (6). Similar to colorectal cancer, there has been a steep rise in breast cancer incidence with economic development and lifestyle change; in Singapore for example, the incidence has tripled since 1960s and a shift from premenopausal to postmenopausal breast cancer has been observed. Greater awareness and mammography likely account for this rise as well.
Gastric Cancer
In 2008, more than 60 per cent of cases worldwide occurred in East Asia. Japan has a high gastric cancer rate, with Korea following close behind. The Japanese diet is characteristically high in salted foods, nitrates and pickling preservatives. Fermentation and the pickling process are believed to interact, playing a significant role in lower vitamin C rates linked to poor immunity and higher cancer incidence. In a population-based prospective study (7) done in Japan, consumption of highly salted food such as salted fish roe and salted fish preserves were strongly associated with an increased risk of gastric cancer. Helicobacter pylori infection, smoking and low consumption of fruit and vegetable are other factors associated with the risk of gastric cancer.
Liver Cancer
The major risk factors for liver cancer include chronic infection with Hepatitis B and C in the setting of liver cirrhosis, the consumption of foods contaminated with aflatoxin and heavy alcohol consumption. In 2008 male incidence rates ranged from 3 per 100,000 in South-Central Asia to 36 per 100,000 in East Asia, and female rates ranged from 2 per 100,000 to 13 per 100,000 in the same regions. With high rates of Hepatitis B and C infection and widespread alcohol use, Mongolia has the highest incidence rates of liver cancer by far (117 and 75 per 100 000 in males and females respectively).
Cancer Prevention and Screening
The World Health Organization states that the global burden of cancer can be reduced and controlled by implementing three evidence based strategies: preventing cancer from occurring in the first place, early detection, and better management of patients with cancer.
Prevention of Cancer
Tobacco use is the single greatest avoidable risk factor for cancer mortality in Asia and worldwide. Tobacco smoking causes many types of cancer. Anti smoking campaigns have been launched in many countries in Asia. In China, several programs are ongoing (4). China signed the WHO Framework Convention on Tobacco Control in 2003 and ratified it in 2005. And In 2008, China became the first country to host the Olympic Games since the Convention came into effect and organized a complete smoke-free green Olympic.
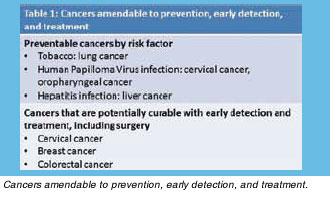
Infectious agents are responsible for many cancer deaths in developing countries in Asia. Hepatitis B causes cancer of the liver, Human Papilloma Virus causes cervical cancer and squamous cell oropharyngeal cancer, and Helicobacter Pylori bacteria increases the risk of gastric cancer, Preventive measures include vaccination and prevention of these infections. In Korea, the first national Hepatitis B Virus (HBV) vaccination program began in 1985 and by 1995 the HBV vaccination program was integrated into the routine childhood immunization schedule (8). In China, vaccination of infants against Hepatitis B was initiated in 1992. In June 2009, China launched a program giving booster shots of HBV vaccine to those under the age of 15 (9). In Taiwan, since the launch of HBV vaccine in 1984, the national hepatitis B vaccination program has been successful in preventing acute and chronic liver diseases and has continued to be a mainstay of their national health program (10). In 2006, Mercks Gardasil received approval from the US Food and Drug Administration, recommended for girls and women aged 11 to 26. However, the uptake rate was not high. Currently, the prevalence data for the general female population and some population sub-groups, such as young females, are insufficient thus questioning the cost-effectiveness of the vaccination delivery and education. The current vaccine only prevents about 70% of cervical cancer cases and will take years before a reduction in the incidence of cervical cancer can be seen (11). Therefore, screening detection from pap smear still plays an important role (Table 1).
Other environmental factors can be modified to reduce cancer risk, including adopting healthy diets, controlling obesity and exercise. Working towards healthy building a healthy environment is an inexpensive way that both developed and developing nations in Asia can do to reduce cancer burden .
Screening of Cancer
Although a variety of programs on cancer prevention and control are being carried out in Asia, there is still a long way to go. Only a small proportion of cancers are inherited, thus, most cancers cannot still be predicted, and screening remains the main mode of early detection (Table 1).
Gastric Cancer Screening
Gastric cancer is a leading cause of death from cancer in Japan and Korea. Since 1983, gastric cancer screening has been conducted nationwide in Japan for all residents aged 40 years and over (12). By contrast, the relatively low incidence of gastric cancer in other regions makes this strategy costly and unwarranted. In low risk regions, case-finding rather than mass screening is the most appropriate approach for early detection.
Colorectal Cancer Screening
Colorectal cancer is now the second most common malignancy in many Asian countries, and in some places the incidence, distribution, and mortality rates of the disease are similar to those of the West. This increase may be due to rapidly changing lifestyles and diets. With rapidly rising incidence, a natural history of progression from polyp to cancer makes it very suitable for screening programs targeted to the general population. National guidelines on colorectal cancer screening are nonexistent in most Asian countries except in Japan, Korea, Taiwan, and Singapore (13).
Breast and Cervical Cancer Screening
Early breast cancer detection through mammography has been shown to increase treatment options and save lives, and has been recommended in countries like Singapore. Recommended early detection strategies in some developing countries include the promotion of awareness of early signs and symptoms and screening by clinical breast examination. In Taiwan, the national screening program for cervical cancer has been successful in reducing the rate of cervical cancer risk (14).
Conclusion
Asias burden of cancer is predicted to increase largely because of the better and earlier screening detection methods, longer life expectancy and an aging population trend in developed countries and in economically developing countries, an increase in adoption of cancer-causing behaviors, in particular smoking and dietary habits. As the rates of cancer increase in Asia, this is a major health problem, as well as a challenge to the health system in each country in Asia. Many people in the developing countries have no health insurance and many are too poor to go for screening tests. And many more are too poor to afford the treatment for the Cancers amendable to prevention, early detection, and treatment.cancers. It is important for the health organizations in each country to realize this epidemic of cancer and to reduce the incidence of cancers by simple primary preventive measures such as tobacco abstinence, changing diet, weight and lifestyle. The cornerstone is a comprehensive multidisciplinary approach focused on education, cancer prevention and screening to management of disease, rehabiliation and palliative care. This requires the amalgamation of efforts of hospital and private practitioners, medical insurance companies, government bodies and media (15).
 Click here to download the full issue for USD 6.50 Click here to download the full issue for USD 6.50
|